
 Members of The Church of Jesus Christ of Latter-day Saints who understand the Church’s position on abortion or the reasons for its emphasis on the family and the sanctity of human life need to be better prepared to talk to our children, our fellow members, and many others about the issue of abortion. As we listen gently to their sincere questions or concerns, we must also find the right moments to teach based on sound doctrine but also sound science. The science part, if we are prepared, might be helpful in addressing the emotionally charged talking points that they have heard.
Members of The Church of Jesus Christ of Latter-day Saints who understand the Church’s position on abortion or the reasons for its emphasis on the family and the sanctity of human life need to be better prepared to talk to our children, our fellow members, and many others about the issue of abortion. As we listen gently to their sincere questions or concerns, we must also find the right moments to teach based on sound doctrine but also sound science. The science part, if we are prepared, might be helpful in addressing the emotionally charged talking points that they have heard.
Many young people, like a faithful daughter-in-law of mine, were told repeatedly in their education that an unborn baby is not yet human. In fact, a biology teacher at her high school had told her that the fetus is actually a “parasite” and even at birth, it’s not really human yet and takes time to gradually start becoming like a real human.
She had long planned on having only one child, but when that first child came, when she saw the beauty and precious innocence of the vividly alive infant freshly freed from her womb, so clearly and fully human, she was not only amazed but also outraged at the scientific misinformation she had been given. That child had more than just a brain—she had a personality. She had been moving and kicking inside her for many weeks, responding to motion, to voices, to the world around her, and very little had changed by passing through the birth canal. What had been within the mother’s body was the same gorgeous creature that was now in her harms, a precious but vulnerable human being with its own nervous system, its own immune system, its own beating heart, its own fingerprints—in every way a separate human being and a separate soul, in spite of having been dependent on the body of the mother, a dependency that would continue for months to come and that is irrelevant to the debate over whether that infant should have the right as a human being to live and be protected from harm.
But the real outrage came after she noticed how the baby recognized her and how deeply that infant loved and trusted her—the infant she might have unwittingly killed:
My outrage mainly centered around the fact that not only was she human but she trusted me more than anyone. I was able to comfort her when no one else could. The thought that it could have been me that terminated her life was emotionally terrifying—like what if I had done something like that and then later had a baby who trusted me? How could I have lived with that knowledge?
My daughter-in-law had been lied to over and over by authority figures in her education and by other influencers. Thank goodness the Gospel had helped her have the faith to bear a child. That faith has continued to grow, one miracle at a time, and has led her to withstand the pressures of society and to go on to bear more children, each a unique, precious soul with the potential to make the world a better place. The challenge for her and all of us is to give our children the faith and intelligence they will need to realize their potential, to have joy, and to withstand the deceptive teachings of others on the most sacred matters of all, including the sanctity of life.
Many people who feel upset over the Supreme Court decision that has overturned Roe v. Wade have heard that this decision will cause women to die. They have heard that abortion on demand at any time prior to the child being fully born is an essential part of health care for pregnant women and unrestricted access to abortion makes the world a healthier, safer place for women. Here I won’t quibble over the large elephant in the room, or rather, the small human in the womb, but wish to point out what science actually tells us about maternal health and abortion. This information is easy to find if you know what to look for and avoid the censorship of Google and other social media sources. For search engines, I now recommend some you may not have heard of, but which both protect your privacy and seem less likely to censor search results based on Google’s “progressive” agenda. My recommendations are Swisscows.com, Presearch.com, and Brave.com. So let’s look at the science.
In 2017, a study was published that looked at hundreds of available studies dealing with maternal health, and found that eleven had enough information to yield conclusions about the health of women following termination of pregnancy (including miscarriages and abortion) relative to those who went through childbirth. The published paper is David C. Reardon and John M. Thorp, “Pregnancy associated death in record linkage studies relative to delivery, termination of pregnancy, and natural losses: A systematic review with a narrative synthesis and meta-analysis,” SAGE Open Medicine 5 (2017): 2050312117740490, DOI: 10.1177/2050312117740490. Here is an overview:
Objectives:
Measures of pregnancy associated deaths provide important guidance for public health initiatives. Record linkage studies have significantly improved identification of deaths associated with childbirth but relatively few have also examined deaths associated with pregnancy loss even though higher rates of maternal death have been associated with the latter. Following PRISMA guidelines we undertook a systematic review of record linkage studies examining the relative mortality risks associated with pregnancy loss to develop a narrative synthesis, a meta-analysis, and to identify research opportunities.
Results:
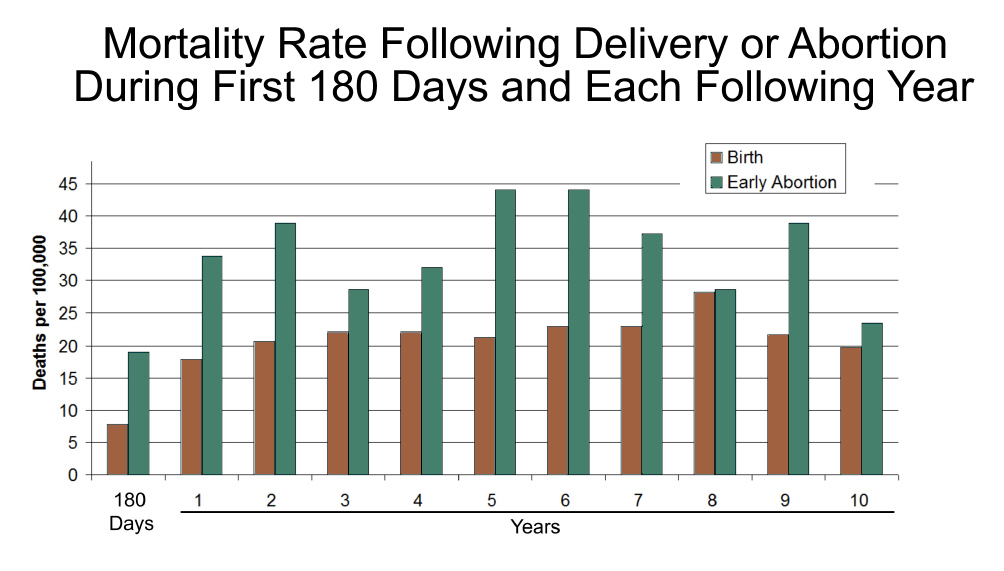
Of 989 studies, 11 studies from three countries reported mortality rates associated with termination of pregnancy, miscarriage or failed pregnancy. Within a year of their pregnancy outcomes, women experiencing a pregnancy loss are over twice as likely to die compared to women giving birth. The heightened risk is apparent within 180 days and remains elevated for many years. There is a dose effect, with exposure to each pregnancy loss associated with increasing risk of death. Higher rates of death from suicide, accidents, homicide and some natural causes, such as circulatory diseases, may be from elevated stress and risk taking behaviors.
[emphasis mine]
Eleven different studies from three nations show that if a woman is pregnant, she will be less likely to die if she completes the pregnancy. (That’s an average result that may not apply to every specific group.) Why the higher death rate? Multiple factors are involved. Here are some mentioned in the Reardon study:
Compared to women who deliver, those who miscarry or have TOP [termination of pregnancy] face significantly elevated rates of psychiatric disorders,2–10 substance use,5,6,10–13 suicidal behaviors,5,6,13–16 sleep disorders,17 post-traumatic stress disorders,7,18,19 a decline in general health,20 and elevated rates of recourse to medical treatments in general,21,22 most of which have been observed within the first through ten years following the pregnancy loss. Any and all of the aforementioned conditions may shorten longevity. It is therefore especially important from a public health and economic viewpoint to improve investigations regarding the mortality rates associated with pregnancy losses.
Note that these studies don’t mean that abortion directly causes the adverse health effects. In fact, Reardon’s paper notes that a key risk factor is violence:
While the risk of death after pregnancy loss is most elevated in regard to deaths from violent causes,87,92 there is also evidence that when risk of death after pregnancy loss is tracked beyond one year a significant higher risk is also associated with specific causes of natural death, such as circulatory disease.
So perhaps part of the problem is that women with abusive boyfriends or living in more violent parts of town might be more likely to have an abortion. Indeed, in the US, lower-income neighborhoods are a key focus for Planned Parenthood’s abortion clinics. But Reardon also notes that “the risk of death associated with pregnancy loss remains elevated even after controlling for psychological differences and economic class.92“
The first five contributory factors mentioned above may all be related to mental health and seem particularly important: psychiatric disorders, substance use, suicidal behaviors, sleep disorders, and post-traumatic stress disorders. A consequence of abortion for many women that is rarely discussed in the mainstream media is painful regret. I’ve heard such regret from women I’ve known and from others sharing their story. Their neglected voices need to be considered in a society that is quick to applaud abortion as if it were some badge of courage or a glorious rite of passage. Not all may report this, of course, and some claim to have been liberated and made much better off by their abortion. But the anguish some women may feel, perhaps especially when they were pressured by others (a boyfriend, family, friends, teachers) into doing something that seemed wrong can contribute to depression, suicidal thoughts, etc. They need love and understanding. For some, the anguish becomes even greater when they find, as some have found, that the abortion has reduced or destroyed their chances of having a baby later. (Such potential side effects may not have been disclosed.) For my daughter-in-law, just thinking about how easily she could have been misled into killing her beloved daughter, a being that totally trusted her and loved her and depended on her for life, filled her with terror. Those who have undergone abortion need comfort and love, and especially need the hope and freedom from sin that the Gospel of Jesus Christ brings. Those who made the mistake of having an abortion remain daughters of God whom He loves and wishes to forgive through the power of Jesus Christ. His love and mercy are available and desperately needed. We must do a better job of bringing the Gospel message of true love and forgiveness to a world misled in ways that eventually bring profound guilt and pain.
Reardon recognizes that “correlation is not causation,” but discusses one factor that may contribute to these mental health and stress-related issues: the potential of coercion to have an abortion:
Another factor to consider regarding the question of causality is that negative effects may be substantially limited to small subgroups of women who are at greater risk. For example, experts on “both sides” of the legal abortion controversy are actually in agreement regarding the evidence that women who feel coerced or pressured into unwanted TOP are at greater risk of serious complications, including elevated self-destructive tendencies.98 If we were to hypothesize, then, that all of the elevated risk of death associated with TOP [termination of pregnancy] reported in the studies we examined are limited to cases of coerced TOP, it would then follow that the findings reported herein may be an indirect measure of the frequency of coerced TOP. Such a conclusion would only further underscore the importance of the clinical recommendations offered in the next section.
Perhaps the most powerful evidence that pregnancy loss contributes directly to mental health problems is the frequency with which self-aware, introspective women specifically attribute the onset or worsening of substance use, depression, flashbacks, sexual dysfunction, self-destructive tendencies and other issues to their pregnancy loss experiences.93,99,100 These self-assessments are further validated by therapists treating women for pregnancy loss related issues.101,102 Additionally, evidence that post-abortion counselling programs reduce symptoms of psychological illness103 also support the hypothesis that TOP can trigger or exacerbate psychological illness; after all, an effective treatment is evidence for an accurate diagnosis.
We are not asserting that pregnancy loss is the sole cause of the elevated risk of death identified in these studies, but rather that there is ample evidence to believe pregnancy loss can be a contributing cause. The discussion above is therefore intended to emphasize the importance of research designed to better understand the causal pathways and co-occurring risk factors which can then be used to better identify women who may benefit from appropriate interventions.
[emphasis mine]
Here’s a little more detail from the Reardon study, explaining how the criteria for the study resulted in whittling down numerous studies on maternal health to the eleven studies with adequate information for the analysis:
A total of 68 studies examining populations in 11 countries met the criteria for the first level of eligibility. All of the studies identified significantly more maternal deaths than would have been identified by reliance on death certificates alone.
Of the 68 studies identified, 57 included record linkage of only birth and death records. In other words, they lacked any data on deaths associated with pregnancy losses. The distribution by country of these studies was as follows: one in Bangladesh,28 one in Brazil,29 two in Canada,30,31 one in Denmark,32 one in Italy,33 three in Netherlands,34–36 four in Sweden,37–39 one in Taiwan,40 six in the United Kingdom,41–46 thirty-four in the United States including Puerto Rico,47–79 and three reporting data from multiple countries for which at least one country’s data used record linkage which met our criteria for inclusion.80–82
The remaining 11 studies met the criteria for the second level of eligibility: reporting results of linkage of death certificates to independent records of pregnancy loss. These included seven studies from Finland,1,83–88 two from Denmark,89,90 and two from the United States.91,92 Two of these investigated only deaths in the year following TOP.88,91 The remainder investigated pregnancy associated deaths and/or pregnancy associated long-term mortality relative to both birth and pregnancy loss.
Here’s a graphical view of the results:
The eleven studies discussed by Reardon include:
- Gissler M, Berg C, Bouvier-Colle M-H, et al. Methods for identifying pregnancy-associated deaths: population-based data from Finland 1987–2000. Paediatr Perinat Epidemiol 2004; 18(6): 448–455. [PubMed] [Google Scholar]
- Shelton JD, Schoenbucher AK. Deaths after legally induced abortion linkage. Public Health Rep 1978; 93(4): 375–378. [PMC free article] [PubMed] [Google Scholar]
- Gissler M, Hemminki E, Lönnqvist J, et al. Suicides after pregnancy in Finland, 1987-94: register linkage study. BMJ 1996; 313(7070): 1431–1434. [PMC free article] [PubMed] [Google Scholar]
-
Gissler M, Kauppila R, Meriläinen J, et al. Pregnancy-associated deaths in Finland 1987–1994 – definition problems and benefits of record linkage. Acta Obstet Gynecol Scand 1997; 76(7): 651–657. [PubMed] [Google Scholar]
-
Gissler M, Hemminki E. Pregnancy-related violent deaths. Scand J Public Health 1999; 27: 54–55. [PubMed] [Google Scholar]
- Reardon DC, Ney PG, Scheuren F, et al. Deaths associated with pregnancy outcome: a record linkage study of low income women. South Med J 2002; 95(8): 834–841. [PubMed] [Google Scholar]
-
Gissler M, Berg C, Bouvier-Colle M-H, et al. Pregnancy-associated mortality after birth, spontaneous abortion, or induced abortion in Finland, 1987–2000. Am J Obstet Gynecol 2004; 190(2): 422–427. [PubMed] [Google Scholar]
-
Gissler M, Berg C, Bouvier-Colle M-H, et al. Injury deaths, suicides and homicides associated with pregnancy, Finland 1987–2000. Eur J Public Health 2005; 15(5): 459–463. [PubMed] [Google Scholar]
-
Gissler M, Karalis E, Ulander V-M. Decreased suicide rate after induced abortion, after the Current Care Guidelines in Finland 1987–2012. Scand J Public Health 2014; 43(1): 99–101. [PubMed] [Google Scholar]
-
Reardon DC, Coleman PK. Short and long term mortality rates associated with first pregnancy outcome: population register based study for Denmark 1980–2004. Med Sci Monit 2012; 18(9): PH71–PH76. [PMC free article] [PubMed] [Google Scholar]
-
Coleman PK, Reardon DC, Calhoun BC. Reproductive history patterns and long-term mortality rates: a Danish, population-based record linkage study. Eur J Public Health 2013; 23(4): 569–574. [PubMed] [Google Scholar]
These studies involve a small number of researchers, dominated by Professor Mika Gissler of Finland and others in Scandinavia, and David C. Reardon and his colleagues in the US. Reardon is calling for more studies from more researchers, frustrated that such important data has been so neglected in the literature.
There are many more issues to study here. You can explore the eleven studies Reardon examined, for example, and do more of your own research. There are also other potentially important issues to consider such the issue of infertility after an abortion. For this, you may wish to consider the “Summary Paper on the impact of induced abortion on Women’s subsequent mental and physical health,” deVeber Institute for Bioethics and Social Research, and Carole Novielli’s summary, “It’s no myth: Studies, documents say abortion can cause infertility, miscarriage,” LiveAction.org, July 22, 2018. Some data has pointed to cancer issues (e.g., a meta-analysis of Chinese women and some other earlier reports), but this is not at all clear. The American Cancer Society offers pretty convincing evidence that there is not a demonstrated connection between abortion and cancer.
Censorship?
David Reardon, lead author of the Reardon study, wonders why so few researchers have chosen to report data on adverse health effects in those having abortions. The eleven studies Reardon considers tell us a lot, but there are mountains of additional information that apparently is not being reported. The following comes from “Each Abortion Increases Woman’s Risk of Premature Death by 50%, New Study Reports,” Afterabortion.org, Nov. 14, 2017:
According to the review’s lead author, Dr. David Reardon, the elevated risk of death following pregnancy losses (abortion or miscarriage) was first identified in a study of the entire population of women in Finland in 1997. Reardon is the director of the Elliot Institute, a research group focused on reproductive health issues.
Reardon said that most of the record linkage studies published since 1997 could and should have investigated the differences in maternal death rates relative to pregnancy loss. But most researchers chose to only report on deaths associated with childbirth.
“It’s difficult to believe that these maternal mortality specialists are unaware of the unanimity of the 11 large population studies from Finland, Denmark, and the United States in regard to elevated risks of death following reproductive loss,” he said.
Reardon believes that the lack of more data on deaths following pregnancy loss is most likely due to a bias against publishing results that might undermine international efforts to promote access to abortion in less developed countries.
Apart from the unwillingness of researchers to share the bad news in the data about abortion, Google might not be all that willing, either. I mentioned the use of other search engines above because I had a difficult time finding some studies for which I had related quotes that should have made it easy to find. For example, from the Reardon study, when I searched for “women experiencing a pregnancy loss are over twice as likely to die compared to women giving birth” (without quotes), the Reardon study came in at #8 on Google. With SwissCows.com, it was the first in the list, after an ad. But the first search I did used a sentence from a link from a conservative news source that my wife had sent me discussing the 2017 Reardon study: “In 2017, a peer reviewed systematic analysis showed that every study (11 in total) examining death certificates linked to reproductive health records has shown elevated risks of death among women following abortion.” I thought that ought to be enough to find the study right away. But nothing in the first page of results at Google (nor on the first six pages, after which I stopped looking) was related to the Reardon study, and most links were to articles or reports that fit a progressive narrative. Even using quotes around the sentence didn’t bring up the easily available story in Google. However, when I used that sentence with or without quotes, the article that had been quoted was at the top of the list, as one would expect. Hmm, just a glitch on Google’s servers?
Sharing the Science
If we throw “science” around as a club to batter opponents, little good will be done. But when we are talking with others and listening to them, seeking to understand, we can often find routes to share some new views. “Tell me why you feel that limited abortion on demand will cause women to die?” They may then cite misinformation on ectopic pregnancies or the claim that abortion is vastly safer than pregnancy. Here you may be able to ask if they’ve seen what happens when researchers actually test that hypothesis and compare maternal deaths from those who have had abortions versus those who complete their pregnancy. “You might be surprised to find that every single study from multiple locations examining that gives pretty much the same answer. Would you be interested in knowing what the data really show?”
If they don’t want to know and are irritated at the very thought that you are not a militant Roe v. Wade crusader, there’s no sense in further irritating them. Don’t dismiss your disagreeing friends as bad people who need to be unfriended and never allowed to hang out with you again. Be kind, move to another topic, avoid an explosive encounter, and please remain being a friend. But if they are willing to consider the science, you may be guided to touch them in a helpful way. You can discuss some studies and perhaps show them a good reminder of what science is learning about the unborn child. That might be a good moment to help them visualize what science has shown us, turning to the fascinating “Baby Olivia” video.
You could also share what happened when Dr. Bernard Nathanson, an atheist and director of what was the largest free-standing abortion facility in the world, started examining the human fetus with ultrasonic visualization. He found overwhelming evidence that what he had been aborting was a human being and could react in pain to the gruesome methods of abortion. (The issue of when an unborn child can first feel pain is complex and, of course, hotly contended, but there is now a significant body of scientific evidence indicating that pain may be felt much earlier than abortion advocates will admit.) Horrified at what he learned from scientific observation alone, he resigned and confessed that the industry he had profited from had relied on lies and scientific misinformation to drive the Roe v. Wade decision and gain popular support for abortion. He became a pro-life advocate. See Dr. Mark Houghton’s reply to an obituary for Dr. Nathanson published in the medical journal BMJ for some valuable important perspectives on Nathanson’s work.
Building on what Nathanson learned, you might be able to discuss the science of early human life in the womb to help that the clump of pink cells is a human being, something that should help others recognize that abortion is at least something more serious than trimming a fingernail or yanking a tooth. Then you might get into what the data tells us about the health of the mother. There are consequences to abortion that may be harmful, and there are alternatives when a pregnancy is unwanted such as adoption that can be healthier not just for the unborn child, but also for the mother. You might also warn that there are billions of dollars of profits at stake in this debate, and the abortion industry has huge incentives to deceive with emotionally charged misinformation.
With God’s help and a gentle but informed approach, a heart might begin to soften, a mind might become a little more open, and one day there may be grateful voices thanking you for what you did. But even if you’re unfriended moments later, at least you tried to make a difference in a world in need of your help. Don’t give up.
Closing Remarks
Roe v. Wade was decided in an era when there was abundant ignorance about the nature of the unborn baby, though enough was known to make it clear then that a fetus is human and has a body distinct from the mother’s body. Today, however we know so much more. We know about the rapid development of the infant’s nervous system, hands and fingers and finger prints, its separate circulatory system and immune system, and much more that makes us marvel at the miracle of early human life. We know that an unborn child is much more than a formless clump of pink cells, and we know that the hundreds if not thousands of students over the year at my daughter-in-law’s high school who were taught by at least one teacher that an unborn child isn’t human and doesn’t even look human at birth was dead wrong. We know that many infants are being aborted that could have been viable outside the womb. We know that many babies being aborted with brutal methods can and do feel pain. The scientific misinformation prattled off by abortion advocates is sickening. So many are taught that the baby is not alive, not human until it’s out of the womb, and free game for slaughter.
No pregnancy that I know of was especially convenient. Life comes at a cost that is not to be downplayed. But the data shows us that there are costs to abortion on demand that go beyond the already extreme cost of the unnecessary death of an innocent and precious human being. There also can be costs to the mother. Compared to those who go on to bear their child, the data show a significant increase in health risks that need to be discussed. The claim that any restrictions in access to abortion means more women will die appears to he untrue. It’s horribly untrue on the face of it when we consider that 50% of the victims of abortion are female, but even if we focus on the mother alone, the claim abortion restrictions kill women is unjustified by science. Following the science here could be a matter of life and death.
Related resources:
- “The Annotated Proclamation on the Family,” TheFamilyProclamation.org, https://thefamilyproclamation.org/annotated-proclamation/.
- “Each Abortion Increases Woman’s Risk of Premature Death by 50%, New Study Reports,” AfterAbortion.org, 2017, https://afterabortion.org/each-abortion-increases-womans-risk-of-premature-death-by-50-new-study-reports/.
- The Elliot Institute, AfterAbortion.org.
- David C. Reardon et al., “Deaths Associated With Abortion Compared to Childbirth a Review of New and Old Data and the Medical and Legal Implications,” Journal of Contemporary Health Law & Policy 20, no. 2 (2004): 279-327.
- “Justice Sotomayor is Wrong: Women Are Not Fourteen Times More Likely to Die from Pregnancy,”
Charlotte Lozier Institute, June 24, 2022. - “Fact Check: Dobbs Will Not Impact Life-Saving Medical Care for High Risk or Ectopic Pregnancies,” Charlotte Lozier Institute, June 24, 2022.








It sounds like the same reasoning used to sell us expensive pharmaceuticals. You are twice as likely to be cured of what ails you tkaing our expensive daily pill!
Twice! Wow! Zoom in on the data. Twice means ten instead of twenty out of ONE HUNDRED THOUSAND. I’m sorry, an additional ten is not stats, but rather, anecdotes. If you look at each of the ten you will find extraneous causes. Hence is why we say correlation is not causation. A regression usually takes multiple variables to find the most impactful.
The Freakonomics folks claim to have done regarding the 30% drop in US crime during the 1990s. A strong economy, additional funding for police, more substantial punishment, etc were all factors, but the strongest factor they claim was the legalization of abortion. Supposedly they pursued the data based on evidence from Romania, where abortion suddenly became illegal in an attempt to increase fertility rates with a resulting dramatic increase in crime.
The conclusion is abortion is a great social benefit and blessing from God.
https://freakonomics.com/podcast/abortion-and-crime-revisited/
Sure, we could execute all of the “undesirables” before they commit a crime. That is one way to reduce crime, I suppose, and a more efficient and corporate way to handle a situation. Minority Report anyone? Or we could find other avenues to reduce poverty since it is poverty that seems to be the bigger indicator of crime and not access to abortion.
Steve
Be ye therefore perfect even as your father in heaven is perfect. Our father in heaven sends a global flood to wipe out the “undesireables”, Gomorrah, commands Joshua to kill even the pregnant women in destroying the children of idolaters, and commands beheading so that nations do not dwindle.
Also, a famous lie of Satan is that poverty is the bigger indicator of crime. Far from the truth.
“we could find other avenues to reduce poverty since it is poverty that seems to be the bigger indicator of crime”
Famous lie told by Satan. Crime isn’t your fault, it is not that you covet, have anger issues, addiction, etc, it because you have less in than others, so you are justified.
Fact is Steve, strongest precursor to crime is not being wanted by ones parents as a child, regardless if you live in a developed country in the wealthest time of human history or in the undeveloped one.
I’m surprised those involved in peer review didn’t deny publication or downplay the results. “Publication bias”, especially as it relates to research that challenges politically correct ideologies seems more common in recent years.