
Though I disagreed with some of the arguments made in the film Believer, as discussed in my previous post,
it did help me to better appreciate how serious our problem with
suicide is within the Utah, as well as all over the world, including
right here in China where suicide remains a serious but often
under-reported problem.
Speaking of suicides in China, I
was just a few yards away from a tragic suicide, and would have been
killed myself if I had stepped over into the path of a man who threw
himself from the tall building where I work. It happened a few months
ago where I work while I was casually reading a book one morning before
work. He was only about 30, I think. It was a disturbing scene that strongly affected me for some time, and that was for a total stranger. On the
same day, I received an even more disturbing image on my phone from some
dear farmer friends in Jiangxi Province whose handicapped son had given up and thrown
himself into a river. Two rather gruesome suicides impacting my life on
the same day. How tragic it can be for families and friends of those who
take their own lives.
Our love and kindness is needed for those around
us in order to help prevent suicide, no matter how much we may disagree
with their religious views, their politics, or their lifestyles. Those
who are feeling alone, depressed, or rejected may be vulnerable to
suicide. Kindness and love can save lives. Kindness and love is also
desperately needed for the families and friends of those who commit
suicide, for their trauma and anguish can be devastating.
In
reading some of the studies related to suicide and some of the reports
and arguments dealing with the role of religion and the Church, it has
been interesting to see how complex the issues are and how easy it is
for serious mistakes to be made when one just relies on gut feel,
emotion, and simple assumptions in assigning blame. Too many critics go
no deeper than just noting that Utah has a high suicide rate and
concluding it must be because Utah has lots of “Mormons” (51%)–or
rather, the people often nicknamed Mormons, but properly called members
of The Church of Jesus Christ of Latter-day Saints. Our critics often
think they are making the world better by leading
people away from or out of the Church, but in terms of suicide
prevention, they may be making things much worse.
For
faithful Latter-day Saints seeking to understand the issue of suicide
and wishing to push back on unfair criticism, it is not enough to merely
point out the fallacy when critics assume that Utah’s suicide problem
is due to the teachings and policies of the Church. There are more
intelligent arguments and evidence suggesting that LDS religious
influence can contribute to a sense of shame or rejection among LGB
youth that can plausibly increase their suicide risk. This is a danger
we need to be aware of and work to mitigate with love and kindness.
While religious involvement and especially attendance in religious
services appears to be a strong positive factor in reducing suicide
risk, there are offsetting factors that also need to be considered. It’s
a complicated issue. More work is needed to understand causes and
effects.
Reports pointing to possibly negative impacts from the Church can be found in the following:
- Daniel Parkinson, “Utah’s Escalating Suicide Crisis and LDS LGBTQ Despair,” Rational Faiths, March 14, 2017.
- Daniel Parkinson and Michael Barker, “The LGBTQ Mormon Crisis: Responding to the Empirical Research on Suicide,” Rational Faiths, Feb 25, 2016.
- Benjamin Knoll, “Youth Suicide Rates and Mormon Religious Context: An Additional Empirical Analysis,” Rational Faiths, March 9, 2016.
I
wish to agree with these authors that the obvious problem in our midst
demands action now to help reduce the problem. But some will assume that
the action needed is not just our personal efforts to be kind, but
systematic efforts to get people out of the Church or to reduce its
influence or to dramatically change its policies and teachings. In light
of the strong empirical data on the benefits of religious faith and
religious activity in reducing suicide, such actions would seem to be
misguided. A wise response requires understanding the many factors that
can contribute to suicide before pointing fingers and prescribing
unhealthy cures.
Not to be a pill, but it seems to me
that none of these reports cited above, nor any of the various
criticisms I’ve seen that seek to blame the Church for Utah’s high
suicide rate, has given any serious attention (usually not even a
footnote or mention of any kind) to one of the most important factors
associated with high suicide rates in the United States and around the
world. Have you heard about this? It’s altitude. That’s right, distance
above sea level. Huh? How can that affect suicide?
The Lowdown on High Altitudes and Suicide
A
wide variety of recent studies show that one of the most persistent and
significant factors associated with high suicide is altitude. The
mechanism is still a subject of research, but the lower oxygen levels at
high altitudes can have an effect
on serotonin and while that can be positive for many people, it can
exacerbate or contribute to depression for others. Multiple studies now
point to altitude as having a significant effect on suicide. There is
still more to understand and debate, but this is a noteworthy
development.
See Rebekah S Huber et al. (including Perry Renshaw, mentioned below), “Altitude is a Risk Factor for Completed Suicide in Bipolar Disorder,” Medical Hypotheses,
82/3 (March 2014): 377–381. Huber et al. examined data from
16 states for the years 2005–2008,
representing a total of 35,725 completed suicides in 922 U.S. counties.
They found that those with bipolar disorder (BD) who committed suicide
preferentially did so at high altitudes, and that altitude had a
stronger effect on sufferers of BD than it did on other mental
illnesses.
The first such study I am aware of is C.A. Haws et al. (including Perry Renshaw), “The possible effect of altitude on regional variation in suicide rates,” Medical Hypotheses, 73/4 (Oct. 2009): 587-90, with this abstract:
In
the United States, suicide rates consistently vary among geographic
regions; the western states have significantly higher suicide rates than
the eastern states. The reason for this variation is unknown but may be
due to regional elevation differences. States’ suicide rates
(1990-1994), when adjusted for potentially confounding demographic
variables, are positively correlated with their peak and capital
elevations. These findings indicate that decreased oxygen saturation at
high altitude may exacerbate the bioenergetic dysfunction associated
with affective illnesses. Should such a link exist, therapies
traditionally used to treat the metabolic disturbances associated with
altitude sickness may have a role in treating those at risk for
suicide.
So Haws et al., like other authors, note
that high altitude doesn’t make everyone more likely to commit suicide,
but seems to be a strong factor for those already suffering from serious
mental health issues.
Now a variety of additional studies have been published, with several cited in the Huber et al. article above.
One study of particular interest is that of Barry Brenner, David Cheng, Sunday Clark, and Carlos A. Camargo, Jr., “Positive Association between Altitude and Suicide in 2584 U.S. Counties,” High Altitude Medicine & Biology,
12/1 (April 2011): 31–35; doi: 10.1089/ham.2010.1058. While earlier
studies looked at mean elevation of various states, Brenner et al.
recognized that altitude within a state can vary widely, so they looked
at mean elevation for individual counties. They analyzed the data from
over 2500 counties in the continental United States, giving much higher
granularity than was possible in earlier work. “The higher-altitude
counties had significantly higher suicide rates than
the lower-altitude counties. Similar findings were observed for both
firearm-related suicides (59% of suicides) and nonfirearm-related
suicides. We conclude that altitude may be a novel risk factor for
suicide in the contiguous United States.” Below is an excerpt and a
chart:
Despite a negative correlation (r = −0.31, p < 0.001) between county altitude and the all-cause mortality rate, there was a strong positive correlation (r = 0.50, p < 0.001)
between altitude and suicide rate at the county level (Fig. 1).
Positive correlations were also observed for both firearm-related
suicides (r = 0.40, p < 0.001) and nonfirearm-related suicides (r = 0.31, p < 0.001).
Controlling for five potential confounders (percent of age >50 yr,
percent male, percent white, median household income, median family
income, and population density of each county), increasing altitude
deciles were associated with significantly higher suicide rates…. The
threshold value for increased suicide rates occurred in the range of
2000–2999 ft….
Similar findings were observed for firearm-related suicides, which
comprise 59% (352,052 firearm suicides per 596,704 total suicides) of
all suicides.
Such findings are gradually making it into
popular media, though I suspect that many of us haven’t heard much
about this yet. One very readable and interesting report is Theresa
Fisher, “There’s a Suicide Epidemic in Utah — And One Neuroscientist Thinks He Knows Why,” Mic.com,
Nov. 18, 2014 (a hat tip to Russell Osmond for this article). For a Wyoming perspective, see Joe O’Sullivan,
“Altitude may be major factor in suicide,” Casper Star-Tribune, Sept. 18, 2011. An excerpt follows:
When it comes to suicide in Wyoming, guns often take the blame
as a contributing factor. So does the isolation and flinty
independence of rural culture. But a possible cause now being
looked at appears to be a more important contributor to
self-inflicted deaths: altitude.Researchers at the University of Utah have found a correlation
between how high above sea level people live and per capita suicide
rates. Between 1999 and 2007, Wyoming had the fourth-highest rate
of suicides per capita in the nation, according to the Centers for
Disease Control and Prevention; states in the Mountain West hold
nine of the top 10 spots.The researchers looked at 35 separate factors that could cause
suicide. Using suicide data from the CDC and mapping data by the
National Aeronautics and Space Administration, they found a
distinct correlation between elevation and suicide.“The Rocky Mountain states just jumped out at you,” said Dr.
Perry Renshaw, a professor at the university who took part in the
research. “No matter what we did, the altitude kept coming up with
a significant factor.”The study shows that suicides occur between 60 and 70 percent
more frequently at high elevations compared to sea level, according
to Renshaw.In fact, altitude surpassed both the isolation of rural culture
and the prevalence of gun ownership, both of which come up as
assumed causes for the high suicide rate, according to Renshaw.
Altitude was the second-highest ranking of 35 variables. The only
suicide indicator that ranked higher was being a single mother, he
said.Renshaw, who has spent 15 years studying brain chemistry, said
lower oxygen levels in the brain affect people with depression and
bipolar disorder.
Both of those disorders involve problems with how the brain uses
energy, according to Renshaw. Recent research suggests that the
amount of oxygen a person receives affects their mental faculties
and performance.“In depression, what we find is that there are changes in these
high-energy compounds in the brain,” Renshaw said.While oxygen makes up the same percentage of air at sea level as
it does at high altitudes, atmospheric pressure — the amount of
molecules compressed into one space — decreases with height.That means people take in fewer oxygen molecules with each
breath in a city like Casper, which is a mile above sea level,
compared to someone living at sea level.Comparisons outside the U.S.
To prove the data wasn’t just a fluke, Renshaw and the
researchers looked overseas to prove their hypothesis. They did
this by analyzing suicide rates in a mountainous country with an
elevation that at its highest reaches 6,398 feet: South Korea.“It was exactly the same result,” Renshaw said, referring to a
comparison of suicides in South Korea with the Mountain West. “The
higher you went, the higher the result.”
More recently, the Salt Lake Tribune has reported on the significance of altitude. See Luke Ramseth, “University of Utah research shows high altitude linked to depression and suicidal thoughts,” Salt Lake Tribune, July 18, 2018.
Understanding
the impact of altitude for those facing depression or other mental
health challenges may now help guide medical professionals in better
assisting patients, including single mothers (being a single mother
turned up in one study as just about the only risk factor more
significant than altitude). If nothing else, getting away to a lower
altitude area for a while might be a big help.
A recent publication involving the Andes, not done by Renshaw, also
points to a possible altitude effect, though the authors don’t seem
familiar enough with Renshaw’s work to explain why an altitude effect
might exist. See Esteban Ortiz-Prado, “The disease burden of suicide in Ecuador, a 15 years’ geodemographic cross-sectional study (2001–2015),” BMC Psychiatry,
17
(2017): 342; doi: 10.1186/s12888-017-1502-0. They found that
“Provinces located at higher altitude reported higher rates than those
located at sea level (9 per 100,000 vs 4.5 per 100.000).” A much higher
suicide rate for the high-altitude provinces.
These
studies are significant enough that they really must be considered by
anyone seeking to understand the issue of high suicide rates in the
Mountain West or elsewhere, IMHO.
Parkinson’s Swift Dismissal of Altitude: A Reminder on Interactions
Altitude
actually was mentioned in one of the articles cited above pointing to
the Church as a possible factor in suicides. Daniel Parkinson in the
first and most recent article listed above mocked the idea that altitude
could be an important factor in the statistics pertaining to suicide
rates in Utah (see “Utah’s Escalating Suicide Crisis and LDS LGBTQ Despair,” Rational Faiths,
March 14, 2017). Parkinson is rightfully alarmed at the increase in
suicide rates among young people in Utah. But while he and his
collaborators have considered many factors in their previously published
analysis, they appear to have neglected what may be one of the most
important factors, altitude. Altitude as a factor in suicide is a trend that shows up not just across the
US but across the world. That doesn’t mean that a high population will always have more suicide than a low population, for there are many factors playing a role and human behavior is complicated. But it shows up as a major predictive factor for suicide and should not be overlooked, in my opinion.
Parkinson’s swift dismissal of this factor
is motivated by the fact that suicide rates in Utah have recently shown
an alarming increase, while the altitude obviously isn’t changing:
Utah’s rank in overall suicide rate went up from #11 in 2014 to #6 in
2015. This is one area where we don’t want to be #1 but we are heading
that way. Sorry folks, it’s not the altitude. As far as I can tell the
altitude hasn’t changed lately. Altitude might explain our elevated
baseline prior to these increases but it in no way explains a tripling
of youth suicides nor these alarming trends among other age groups.
That may sound plausible at first blush, but I
was frankly surprised and disappointed by the reasoning here, especially since I expected that Dr. Parkinson should be used to dealing with multivariate analysis and the
very common possibility of interactions between the factors considered.
Instead, he assumes that any effect of altitude will be a constant part
of the baseline and cannot play a role in explaining a change over
time.
Consider an analogy to skin cancer. It’s an easier issue to
consider, I feel, because it’s less emotional than suicide and
religion, and many people already know that higher altitudes have
stronger UV light because the light passes through a shorter distance in
the atmosphere resulting in less filtering by ozone. “UV intensity
increases with altitude because there is less atmosphere to absorb the
damaging rays,” as the EPA puts it. “Colorado, for instance, has one of the highest melanoma rates in the country, likely due to its elevation,” according to the Dana-Farber Cancer Institute.
Now
let’s consider two hypothetical regions with 100,000 people each, one
region at sea level and one in the Rockies. Let’s assume both places
have similar populations each with two groups, a “safer” group of 90,000
people who prefer to stays indoors and wear sunblock and protective
clothing when outdoors, and an “at risk” group of 10,000 people,
initially, who love to engage in unprotected sports and sunbathing. The
safer groups in both regions may have a low level of skin cancer (let’s
say 50 new cases per 100,000 people per year), while the at risk groups
will have higher rates, with the at risk group in the high region having
a significantly greater rate of cancer (let’s say 300 new cases per
year per 100,000 people at high altitude and 100 new cases per year per
100,000 people at low altitude). With these assumptions, the new cases
of skin cancer per year for the whole population of 100,000 people will
be 55 at low altitude (50*90,000/100,000 + 100*10,000/100,000) and 75 at
high altitude (50*90,000/100,000 + 300*10,000/100,000). So there’s the
baseline difference of 20 cases per year.
Now
assume that after 5 years at a steady rate, something happens that
begins increasing the cancer rate in both locations. One scenario is
that the number of people at risk increases. For skin cancer, this could
mean more people abandon their indoors lifestyle and take up dangerous
activities like golf and jogging. I’ll neglect many details such as the
years of delay that can occur between sun exposure and skin cancer and
assume that the skin cancer increase shows up relatively quickly as sun exposure
increases.
Both locations will now have curves with
an upward trend. Will the curves look the same, with the same rate of
increase, differing only by a constant baseline? No. See the numbers shown in Table 1 and the curves displayed in Chart 1. As the
at risk groups increase, the added numbers in the group at high
altitude will experience a greater increase in skin cancer because they
are being exposed to stronger UV. With the same population and
behavioral dynamics going on, the high region will show a greater rate
of increase in the skin cancer rate. It’s not because of some pernicious
unhealthy impact of Rocky Mountain Mormons, but because the altitude
effect magnifies the rate of increase even when all else is the same.
It’s due to just about the simplest interaction imaginable, one of the
many interactions between factors that are part and parcel in the social
sciences, in health care, and in just about any other field where
multiple factors may influence outcomes.
| Table 1 | New Skin Cancers | |||
| Year | Safer Pop. | At RIsk Pop. | Low Alt. | High Alt. |
| 1 | 90,000 | 10,000 | 55 | 75 |
| 2 | 90,000 | 10,000 | 55 | 75 |
| 3 | 90,000 | 10,000 | 55 | 75 |
| 4 | 90,000 | 10,000 | 55 | 75 |
| 5 | 90,000 | 10,000 | 55 | 75 |
| 6 | 82,000 | 18,000 | 59 | 95 |
| 7 | 74,000 | 26,000 | 63 | 115 |
| 8 | 66,000 | 34,000 | 67 | 135 |
| 9 | 58,000 | 42,000 | 71 | 155 |
| 10 | 50,000 | 50,000 | 75 | 175 |
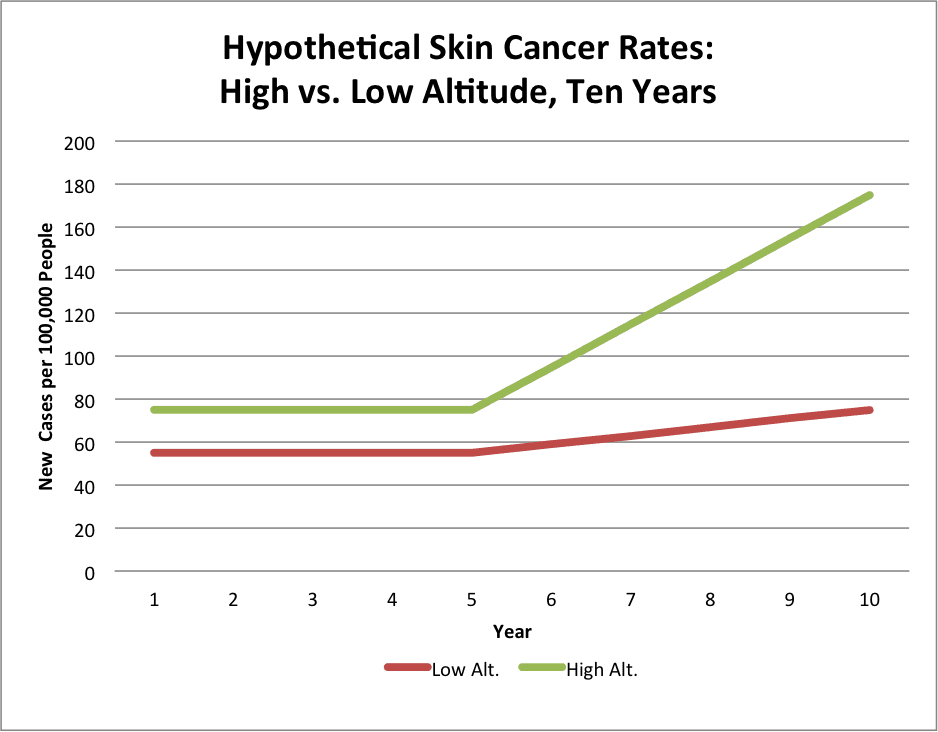
In
the period with increasing skin cancer, the slope (increase in cases
per year) is 20 at high altitude, but only 4 at low altitude. One could
lament that skin cancer has more than doubled in 5 years in the high
altitude location, while showing a much lower increase elsewhere. What
exactly are those lofty high-altitude Mormons doing to spread disaster
in their communities? (Hint: it may not be the Church’s fault!)
Here
we have just about the simplest interaction possible in the data: a
simple relationship between the cancer rate in one group and altitude.
Interactions can be much more complicated and nonlinear, but even a
simple and plausible one results in the kind of differences in rate
between two regions that have caused such alarm and finger-pointing in
suicide statistics. Altitude cannot be neglected, now that multiple
studies have shown it is one of the most important factors in suicide.
When other factors are increasing the overall suicide rate, altitude can
exacerbate the problem, just as it exacerbates the skin cancer rate in
the hypothetical scenario explored above.
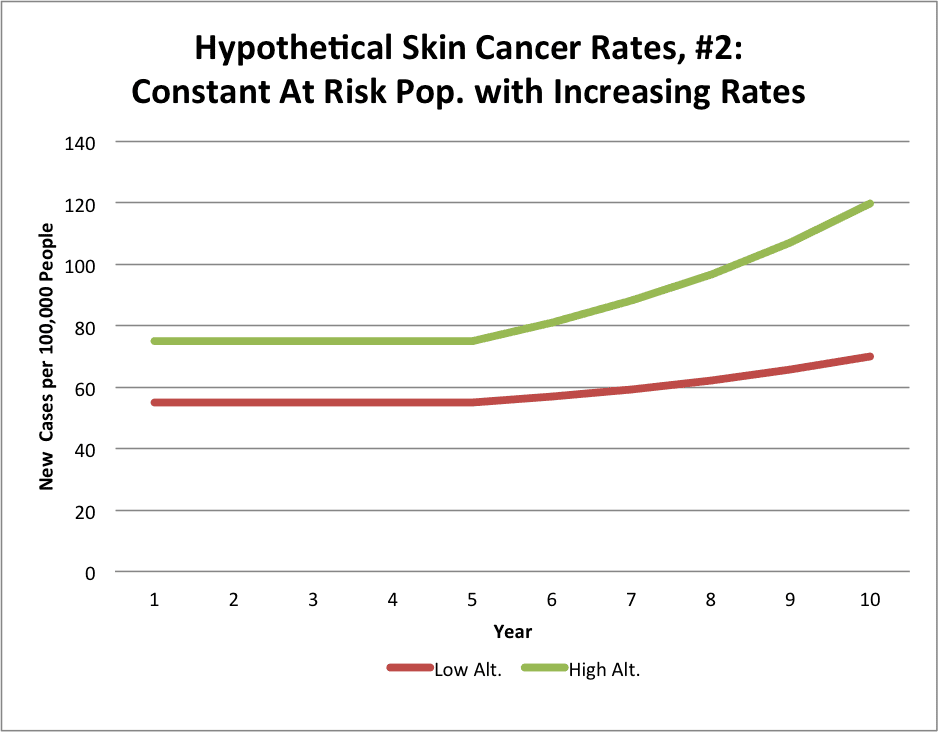
But what if
the size of the at risk population group does not increase in our
analysis above, and instead the rate of skin cancer increases overall
because the at risk group experiences a steady increase in cancer rate
(say, 20% per year) due to environmental factors or some other reason?
Perhaps an interaction with alcohol and drugs, decreasing antioxidants
in diet or legislation that bans the most effective ingredients in sun
block? We can still see similar results.
Here we keep the
two population groups constant (90,000 in the safer group and 10,000 at risk), but in year 5 we begin increasing the skin
cancer rate by 20% a year for both the low and high altitude at risk
populations. The numbers are shown in Table 2 and the curves are in
Chart 2. Here the average slope over the last 5 years ((rate at year 10 –
rate at year 5)/5 years) is 8.93 for the high-altitude location and
2.98 at low altitude, or about 9 and 3, for a 300% difference in the
rate of increase. It’s those Mormons again, no doubt!
| Table 2 | |||||
| Cancer Rates: | |||||
| Year | New Skin Cancers | Safer Group | At Risk, Low Alt. | At Risk, High Alt. | |
| 1 | 55 | 75 | 50 | 100 | 300 |
| 2 | 55 | 75 | 50 | 100 | 300 |
| 3 | 55 | 75 | 50 | 100 | 300 |
| 4 | 55 | 75 | 50 | 100 | 300 |
| 5 | 55 | 75 | 50 | 100 | 300 |
| 6 | 57 | 81 | 50 | 120 | 360 |
| 7 | 59.4 | 88.2 | 50 | 144 | 432 |
| 8 | 62.3 | 96.8 | 50 | 172.8 | 518.4 |
| 9 | 65.7 | 107.2 | 50 | 207.4 | 622.1 |
| 10 | 69.9 | 119.6 | 50 | 248.8 | 746.5 |
My
point here is not just to belabor the obvious error that Parkinson made
in his hasty assumption that any impact of altitude on suicide
statistics could only show up as a simple shift in baseline values and
could not result in a difference in slopes. Rather, I’m calling into
question multiple reports and accusations attempting to paint the Church
as the key cause of high suicide rates or increasing suicide rates in
Utah or in the Mountain West, without having controlled for or
thoughtfully considered the possible impact of altitude.
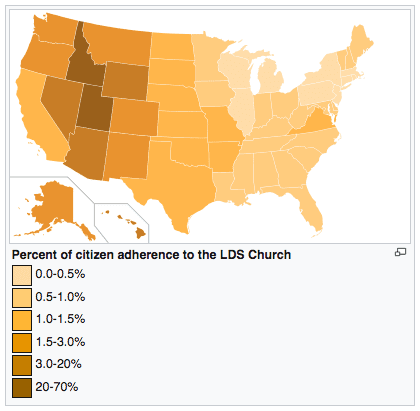
If
you look at the distribution of LDS members based on percentage of the
population in each state, you see a high concentration in the most
mountainous states, as shown in the chart below from Wikipedia’s
article, “The Church of Jesus Christ of Latter-day Saints membership statistics (United States).”
So any analysis of suicide and the relative proportion of Latter-day
Saints in a region could be confounded with the impact of altitude.
Unless altitude is considered in the analysis, the results may be
meaningless and misleading.
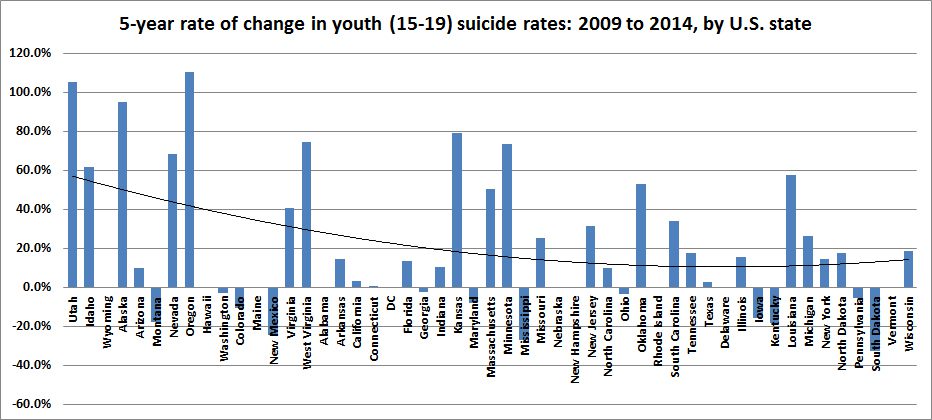
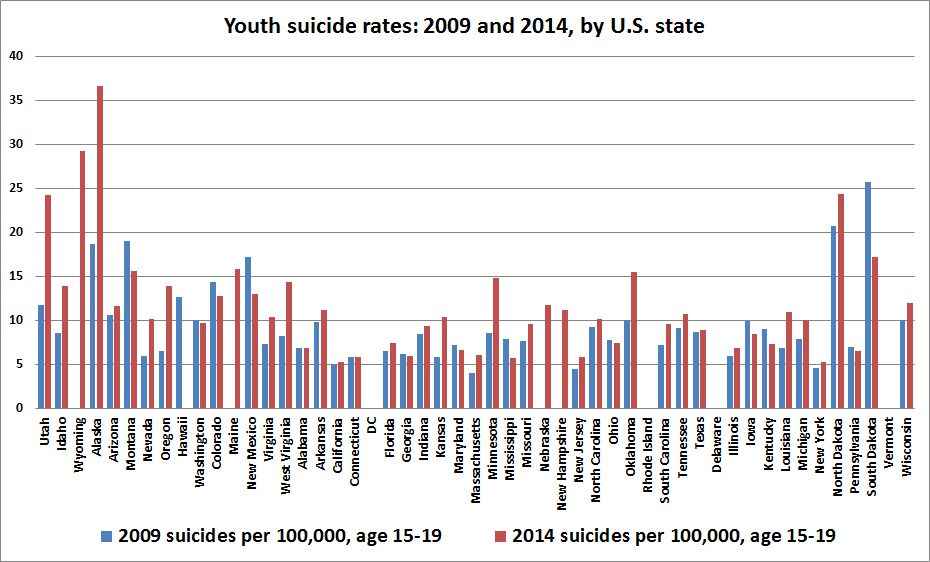
Unfortunately, Benjamin Knoll’s work may be particularly jeopardized by this potential problem. In his report, “Youth Suicide Rates and Mormon Religious Context: An Additional Empirical Analysis,” Rational Faiths,
March 9, 2016, he lists states in order of their LDS percentage, shows
bars for changes in youth suicide rate, and sees an “obvious”
relationship suggesting that the presence of LDS people in a state is
associated with suicide (click the chart below to enlarge). But the
high bars on the leftmost high-LDS end of the graph that support the
curve Knoll has drawn are largely from high-altitude states, or, in the
case of Alaska, have a complex factor of many Native American males with
extremely high suicide rates that may require special consideration in
the analysis.
I’m also puzzled as to how California ends up near the middle with an
LDS influence somewhat less than Alabama or Arkansas, and just greater
than Connecticut. The statistics shown by Wikipedia
put California with a much higher relative LDS population. Something
may be amiss. Further, the apparent 0 bar size for Wyoming is a surprise
since Wyoming has seen suicide increase
at a rate greater than the US national average. Is it apparently zero
because the 2009 data wasn’t found? Maine and several other states seem
to be in the wrong place.
I need to go over Knoll’s data and rerun his analysis, or maybe one of you would like to in your abundant spare time, because I am quite surprised by his claim to have adjusted R2 values of 0.65 and 0.69, respectively, for the relationship between % LDS population in states and the state youth suicide rate for 2009 and 2014, respectively. The data seem scattered all over the place and I just can’t imagine such a high correlation is present. Here is Knoll’s chart (click to enlarge) for these suicide rates (the above chart, recall, is for the rate of change in suicide rates, taking the difference between 2014 and 2009 data). High on both ends with scatter all over. This really gives a strong correlation in both years? But perhaps once controlled for other factors, it pops out. What happens when altitude is added? More work is needed, as always.
Regardless of the problems with
specific
states or other details in this analysis, the failure to consider altitude creates the
risk of confusing
the known effects of altitude for the more speculative effects of LDS
religion in seeking to assess potential causes of the
suicide problem in the US. Whether one looks at current suicide rates or
rates of increase in suicide, altitude can play a role. It really needs to be considered and not dismissed with with a flippant quip.
When the analysis is done more
carefully, there may still be good reasons to worry about LDS influence.
Will those reasons outweigh the known strong positive effects of being
active in religion and in the LDS Church in particular when it comes to
promoting mental health and reducing the risk of suicide? In other
words, will we be helping those at risk for suicide by leading them out
of the Church and keeping them away from LDS neighbors? In the absence
of meaningful data and valid analysis for such a conclusion, I think we
need to be careful about pointing fingers and focus our energy on
encouraging healthy and positive steps by all of us to better support
and love those around us, recognizing that many may be in need of more
support to overcome the pains and burdens they face. On that point, I heartily agree with Daniel Parkinson, Michael Barker, Benjamin Knoll, Dan Reynolds, John Dehlin, and, of course, The Church of Jesus Christ of Latter-day Saints.







Oh! OK. Altitude is a risk factor. So then I suppose if your state is mountainous (though who is actually living in those mountains?) it's a good idea to increase the pressure on vulnerable populations and push them over the edge. Then let the church-sanctioned hate speech continue.
No, those who are vulnerable in any state need help and kindness.
We all know that causation is very difficult to prove. So claims that the LDS Church teachings are causing high suicide rates bewilder me. Is there really any data?
I doubt that persecution is THE factor in such widespread suicide levels. I do not have numbers at my fingertips but I once examined the suicide rates across the country over time. Which demographic is historically at highest risk? Older white males. Blacks historically have had a lower suicide rate than whites, even (as far as we can tell) before the Civil Rights Movement.
Suicide is a serious problem, but I think we should seek data for a historical example of a persecuted population having an extremely high suicide rate. I do not think there is one. Anyone?
Thank you for this careful and well researched post. We need more data, but I'm grateful there are now efforts to try and collect it.
Ask a Utah LDS teen why their friends are committing suicide. I know 2 families who are suffering through this with whom my family are close friends. I will tell you why (fully admitting that my anecdotes do not constitute data, as so few mormons understand): the church's policies and alienation of gay people. Both instances. Ostracism. Shame. Guilt. Being taught that they're bound for eternal damnation.
Not altitude. No soul on earth ever thought back on their loved one who committed suicide and cursed the altitude. I can testify of at least two beloved families who curse the name of the mormon church for leading their children to their untimely deaths.
Suicide comes from within. Outside influences can effect someone’s perception of himself, but ultimately, it’s the individual who is the root cause. The church isn’t encouraging the behavior and is strongly against it—they have long taught that suicide=damnation. Why do we assume that those committing suicide believe the church on one point of doctrine but not on another?
Suicide is a horrible tragedy and we want someone/something to blame for an act, that to those closest to it, is inexplicable, and to all, is senseless. It is caused by mental illness or instability, and should be recognized and treated as such. Blaming social influences is like blaming guns for mass executions, they are part of the equation, but not the root cause of the action.
It isn't necessary to believe any statements of the church if your entire community do and subject you to that sort of judgment. I'm sure it doesn't hurt if you have self-loathing baked in from indoctrination that began before you could speak but even that isn't necessary if you don't have a support system that says "you're good", "you're loved", "we believe in you", "you can expect a future of companionship and love".
After all isn't that how a church community functions and how it enforces group beliefs and behavior?
Tracy Hall Jr. Regarding the correlation of high altitude and suicide, a simple and relatively inexpensive experimental treatment suggests itself. Provide those with depression and bipolar disorder with oxygen during their sleep. Oxygen is a pretty safe drug to use, and the treatment might not even need FDA approval. Oxygen concentrators are available at prices beginning at about $1,500.
Thanks for the post. My heart goes out to everyone impacted by suicide. It is always difficult to have a rational, fact-based discussion with those who emotionally engaged and I see that in the comments above, especially from those those who have lost LDS friends and family to suicide. We always want some understanding of what’s caused the disease or horrible outcome, and for some, blaming the church is an easy source to lash out at. That said, I think the church has done a better job in addressing the issue in recent years and the https://mormonandgay.lds.org website as a major first step.
My cousin was the first person profiled on that website. He says that his attraction to other boys began when he was little — a statement that is typical among my friends who are gay. My cousin talked to his dad and church leaders about his feelings and later served a mission, and I was both surprised and pleased when I saw his picture as the lead story on the Mormon and Gay website. I was also a tad saddened, but not surprised, when my cousin left the church to marry his boyfriend. Homosexuality is something I don’t fully understand, but I recognize its impacts on individuals. My hope is that continued revelation and science will help us all getting a better handle on the issue. I suspect that the impacts of oxygen, altitude, genetics, stress and more can all play a role.
Dr Parkinson argues that altitude can't be relevant because the altitude hasn't changed. Well, neither have the moral standards of the Church of Jesus Christ. If there are indeed those "who curse the name of the mormon church for leading their children to their untimely deaths," then I have to ask: why the need to find a scapegoat?
The church most certainly has picked up the rhetoric on gay members in the last couple decades and hammered it in a way that was merciless and previously unprecedented.
The church simply didn't engage with the issue prior to the '91 challenge to Hawaii's marriage discrimination that woke a sleeping giant. That insensitive giant has been wrecking havoc every since. And actually upping the ante despite their public double speak. The fact is, this roughly corresponds to the alarming rise in suicides in gay LDS youth.
You can continue to refuse to acknowledge it. The suicides will simply continue as a result. And who will answer for that?
It does make me wonder if it would be possible to treat at-risk population groups in high altitude states (people with depression, bi-polar, and other related disorders that seem to be impacted by altitude) by giving them supplemental oxygen, kind of like what's done with CPAP machines for people with sleep apnea.
~Jon
Hhhmmmm….a family member tried to commit suicide….not LDS, not homosexual, and not living in high altitude…. unless 4,000 feet altitude is considered high.
Years later another family member tried to commit suicide….not LDS, not homosexual, and not living in high altitude. This family member was adopted when a week old infant.
So, what was the trigger?
Maybe mental illness and other factors out of their control?
There are stories of people who have grown up in hellish conditions, suffered horrible things done to them by others…. and never tried suicide or turned to drugs or crime, never became horrible people.
Yet, others who grew up in the same conditions and suffered horrible abuses have tried suicide and some were successful, some turned to crime and drugs and became horrible people themselves.
I also personally know of a 30 something female, Mormon, married with children, who committed suicide. To this day the husband does not know what drove his wife to suicide. She did not leave a note or letter; she did not exhibit any suicidal signs or unhappiness, she never let on she would take her own life.
There is more at play than just religion in those Mormons who commit suicide. It's too easy to place blame on something one does not agree with, or place blame on what might seem obvious… but it really is not obvious.
It is complicated and the answers are not obvious…nor easy.
"a 30 something female, Mormon, married with children, who committed suicide"
If she was reading the Book of Mormon regularly, attending church every week, and praying everyday, she would not have committed suicide. If she was unhappy, it is only because she was not living the gospel.
Anon @ 9:06,
Anon at 9:25, there are factors that even the most faithful experience in mortality that can bring great sorrow and depression. Many setbacks and disappointments in life, as well as many forms of mental illness, can lead to despair and hopelessness, and in dark moments, good people who were reading and praying faithfully can succumb to suicide. It is a tragedy that affects some who sincerely seek the Savior, and they deserve our compassion and love.
There are many very good people who succumb to suicide, and I trust the Lord to be tender and merciful with them on an individual basis.
https://www.news-medical.net/news/20180627/Suicide-at-higher-altitudes-unlikely-to-be-caused-by-hypoxia.aspx
"Those that claimed a relationship to altitude and suicide also created a narrative that hypoxia was a significant cause." But when Honigman and his colleagues factored in social isolation, rural living, and access to guns into their analysis they arrived at a different conclusion.
Is not about jumping from one relationship to the other, when you find a true love do everything you can to keep it going because heartbreak can make you lose your mind and unfocused in life. I have experience it and I know how it feels to lose someone you love to somebody else, let me tell you about myself, I got married to a man I love but something happened and we got separated I at first I thought I could coupe but as times goes by, I find out I could not then I realize I needed help to fix my relationship with my husband again that is how I got to know about Dr Ekpen the spell caster who helped me to cast a love spell to get my husband to love me again. In case you are having challenges in your marriage/relationship you can contact Dr Ekpen today to help via: (ekpentemple@gmail.com) or on whatsapp +2347050270218.